


Summary
The functional movement screen, or FMS, is a protocol practitioners use to help identify movement limitations, asymmetries, and compensation patterns that may affect how an athlete trains, performs, or returns from injury.
The FMS is a screen, not a diagnosis. It can show that an athlete struggles with a movement pattern, such as a squat, lunge, or shoulder mobility test. But it doesn’t explain the exact cause of the problem. That requires further assessment and the practitioner’s clinical or coaching judgment.
The FMS is also different from the selective functional movement assessment (SFMA). Both were developed by Gray Cook and Dr. Lee Burton, but they serve different purposes. FMS is used to screen people who aren’t currently in pain. SFMA is a diagnostic tool used by healthcare professionals to assess people who have pain or injuries.
Although the protocol is widely used, it’s not fully objective. Its 0-to-21 composite scoring system depends on how practitioners observe, cue, and interpret each movement. As a result, two trained raters may score the same athlete differently, especially when movement execution isn’t standardized or when the scoring criteria leave room for judgment.
For teams and sports organizations that use the FMS across many participants or locations, that variability creates a challenge: how do you make movement screening consistent enough to trust over time?
In this article, we’ll explain how the FMS protocol works, including the seven tests, the composite scoring system, and how practitioners use FMS scores in athlete assessment. We’ll then examine what the research says about the limitations of the FMS, look at the modern sport-specific athlete movement assessments many practitioners are turning to, and show how markerless motion capture supplies objective 3D kinematics for whatever movement assessment you choose to run.
The Seven Tests of the Functional Movement Screen
Each movement pattern is scored on a scale of 0 to 3. Scoring at each level will look slightly different depending on the movement being performed, but generally:
- A score of 3 means the person was able to perform the pattern as directed.
- 2 means they were able to perform the pattern with compensatory movements or poor mechanics.
- 1 means they weren’t able to perform the pattern at all even with compensations.
- 0 means they experienced pain during any part of the movement.
If the subject experiences any sort of pain or discomfort, the practitioner gives a score of 0 regardless of the quality of their movements.
1. Deep Squat
This involves whole body mechanics and neuromuscular control, and assesses one’s bilateral, symmetrical, and functional mobility, the stability of their hips, knees, and ankles, and motor control of one’s pelvis and core. Holding a dowel above the head requires stability from the shoulders, scapular region, and the thoracic spine.
A score of 3 for the Deep Squat means the person’s heels stayed on the ground, their hips went below parallel (the top of their knees), the dowel remained overhead without tilting forward, and their torso stayed upright.
2. Hurdle Step
This movement is considered integral to locomotion and acceleration, and assesses how the body steps and strides with a dowel along the shoulders while testing the body’s ability to maintain stability and control in a single-leg stance. The Hurdle Step requires bilateral mobility, stability, and control of the hips, knees, ankles, pelvis, and core.
A score of 3 means the hips, knees, and ankles were aligned and the dowel remained level as the person stepped over the hurdle with a single leg.
3. Inline Lunge
This test places the body in a position to simulate the stresses experienced during rotational, lateral, and decelerating movements. The person’s lower extremities are in a split-stance while the upper extremities are in a similar position but in an opposite or reciprocal pattern, replicating a natural counterbalance that demands spine stabilization. The pattern also evaluates the mobility and stability of the torso, shoulders, hips, ankles, feet, and the flexibility of the quadriceps and rectus femoris.
A score of 3 for the Inline Lunge means the dowel remained in contact with the back, including the head, upper back, and sacrum. The movement must be controlled with the person touching their knee to the floor without losing balance.
4. Shoulder Mobility
This pattern evaluates a person’s bilateral shoulder range of motion, combining extension, internal rotation, and adduction in one extremity, and flexion, external rotation, and abduction in the other. It also demonstrates the natural complementary rhythm of one’s scapular-thoracic region.
A score of 3 for Shoulder Mobility means a person’s fists came within one hand length (thumb to middle finger distance) of each other when behind their back. They also must place their hand on the opposite shoulder and elevate their elbow without feeling any pain.
5. Active Straight-Leg Raise
This evaluates a person’s ability to move one leg independently or dissociate their lower extremities, while maintaining a stable pelvis and torso. The pattern also tests a person’s mobility of the opposite hip and their lower abdominal stability.
A score of 3 for the Active Straight-Leg Raise means the person’s non-lifting leg remained flat on the ground while their raised leg achieved an angle of 80 degrees or greater with the dowel aligned between their mid-thigh and hip crease.
6. Trunk Stability Push Up
This pattern isn't a test of upper body strength, but rather an observation of a person’s ability to stabilize their spine in the sagittal plane during an upper body symmetrical movement. The goal is for the person to only rely on their upper extremities to push themselves up while keeping their spine and hips still and steady. Men should be able to perform a push up with their thumbs at forehead level, and women should be able to perform a push up with their thumbs at chin level.
A score of 3 for the Trunk Stability Push Up means the person was able to complete a push up with their body moving as a unit without sagging or compensations.
7. Rotary Stability
This movement requires proper neuromuscular coordination and energy transfer through the torso. It challenges a person’s ability to stabilize their core, multi-plane pelvis, and shoulder girdle when completing a combined, asymmetrical upper and lower extremity movement.
A score of 3 for the Rotary Stability pattern means the person performed a perfect ipsilateral (same-side) movement while keeping their body aligned without wobbling or compensations. A score of 2 for the Rotary Stability pattern means the person performed a contralateral (opposite-side) movement successfully or experienced minor issues during the ipsilateral movement.
The Shoulder Mobility, Trunk Stability Push Up, and Rotary Stability movements all include clearing tests that are scored as pass/fail. If a participant fails the clearing test, they’ll receive a 0 as their overall score for the movement pattern.
How the Composite Score Drives Decisions
A participant’s composite FMS score is often used as a broad summary of movement quality and possible injury risk. A total score between 17 and 21 is typically interpreted as strong baseline movement, while a score between 15 and 16 may suggest minor limitations or asymmetries. A score of 14 or below is commonly cited as a threshold associated with potentially higher injury risk.
The composite FMS score is best treated as context rather than a definitive injury-risk prediction. The individual movement scores, especially 0s, 1s, and left-right asymmetries, are often more useful for deciding where further assessment or corrective work may be needed.
Composite and individual FMS scores can also inform corrective exercise programming and return-to-play conversations, but they shouldn’t be used in isolation. For athletes returning from injury, practitioners may compare current FMS results with pre-injury baselines, while also considering sport-specific testing, strength measures, symptoms, workload, and clinical judgment.
What the Research Says About the Functional Movement Screen
The FMS is widely used, but a decade of research has raised concerns about whether it predicts injury and whether it captures the demands that matter most in sport:
- A 2015 meta-analysis of active adults found poor injury-prediction performance. Specificity was high (85.7%) but sensitivity was low (24.7%), PPV was 42.8%, and AUC was 0.587, leading the authors to conclude that the evidence doesn’t support the FMS as a predictive injury tool.
- A systematic review with meta-analysis found the association between FMS scores and injury too weak to recommend the screen for injury prevention, with moderate evidence against its use in soccer and limited or conflicting evidence across other populations.
- Another review found that FMS composite scores are remarkably similar across high school, collegiate, and professional athletes, clustering around 14 to 16 even though injury rates rise with level of play.
- Reliability is stronger for the composite score than for some individual subtests; in novice raters, the FMS showed moderate-to-good reliability overall, but agreement varied across component tests, making item-level judgments less stable than the total score.
- The FMS evaluates general fundamental patterns and largely ignores deceleration and the external forces an athlete absorbs when cutting, landing, or braking, which are among the most common mechanisms of serious injury.
This isn't to detract from the value of the FMS. It remains an accessible entry point and a common shared language for movement screening. But the evidence has pushed many practitioners toward assessments that more closely mirror the demands of sport.
Modern Alternatives to the FMS
If the goal is to understand how an athlete handles the demands of their sport, assessment should move closer to the movements the sport actually requires. This is the logic behind sport-specific athlete movement assessments, an approach that has grown alongside critiques of the FMS.
Sport-Specific Athlete Movement Screens and Assessments
Unlike the FMS, which is a single, standardized battery of seven tests, a sport-specific movement assessment is more of an approach than a branded protocol. The practitioner selects the movements an athlete actually performs in competition, then evaluates the quality and mechanics of those movements.
The movements most commonly assessed this way include:
- Running and acceleration, where stride mechanics and hamstring loading reveal a great deal about readiness and risk.
- Cutting and change of direction, where knee valgus and trunk control are closely linked to ACL injury.
- Deceleration, a braking action that sits behind many non-contact knee injuries.
- Vertical and lateral jumps, where takeoff and landing asymmetries expose limb-to-limb deficits.
- Single-leg balance, a simple window into stability and neuromuscular control.
Examples From the Literature
The peer-reviewed literature offers validated tools for assessing these movements, including:
- Cutting Movement Assessment Score (CMAS), a qualitative screen that flags high-risk cutting mechanics.
- Qualitative change-of-direction assessments, tied directly to ACL injury risk, with visible knee valgus during cutting associated with roughly 4.6 times greater odds risk of a second ACL injury.
- 2D scoring systems for the deceleration task, which identify athletes with high knee-joint loading.
- Established change-of-direction performance tests, such as the 505 and modified 505, the CODAT, and the Illinois agility test, are also routinely used in return-to-sport batteries.
These qualitative and 2D screens are typically validated against 3D motion analysis, long the gold standard for movement assessment. Producing that data has traditionally meant a marker-based lab setup, but markerless technologies now aim to deliver comparable 3D kinematics much more accessibly.
The NBA's league-wide biomechanics program, detailed further below, is an example and is built around scripted, sport-specific movements rather than the FMS.
How Theia3D Captures 3D Kinematics for Any Movement Assessment
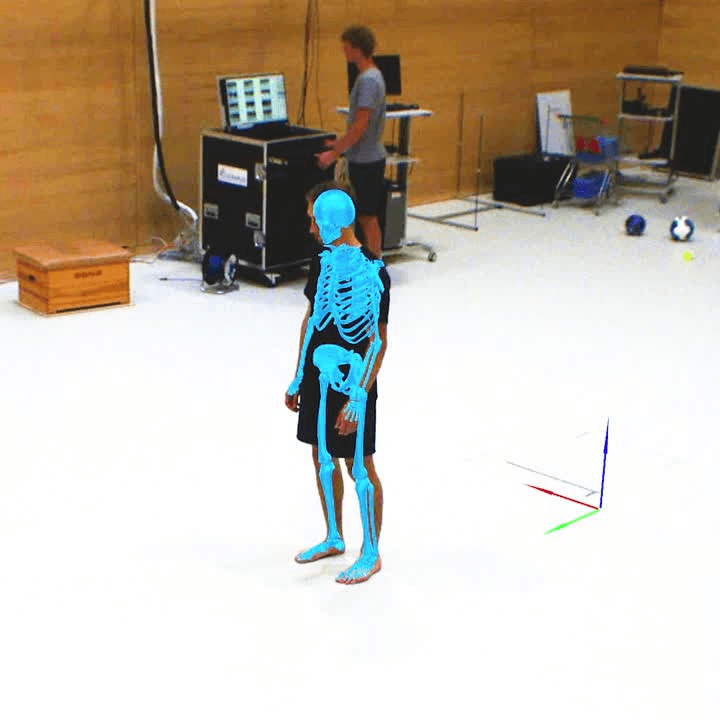
Theia3D takes synchronized multi-camera video and turns it into a precise 3D skeletal model of subjects, with no markers, wearables, or special clothing required.
The software produces objective joint-angle, segment-position, and left-right difference data captured at frame rate, giving practitioners a quantitative record of whatever movement task they capture. Theia3D isn't a screen and doesn’t replace practitioner observation, but is a measurement tool, so the choice of which movements to assess and the interpretation of the data remain entirely with the qualified professional. It also identifies over 120 anatomical landmarks automatically.
Practitioners can set Theia3D up wherever it’s possible to physically mount multiple cameras. Users have, for example, recorded data for analysis in Theia3D at outdoor and indoor tracks, rinks, gymnastics centers, retail spaces, sidewalks, and more.
Theia3D requires eight well-placed cameras to record fully synchronized and high-quality video. The cameras should synchronize video recording both among themselves and with signals from external devices like electromyography sensors, force plates, and instrumented treadmills.
To calibrate the cameras, Theia3D offers a custom proprietary board for participants to use in the capture area, or they can simply record a short video of someone waving a standard active wand. After that, subjects perform the selected movement tasks as directed.

An important point to note is that the software is post-processing and doesn’t offer real-time person tracking.
Capturing Natural Movement as Objective Kinematic Data
Theia3D takes significantly less time than a marker-based system to get started, as no sensors or reflective markers need to be attached to participants.
Athletes perform the chosen assessment exactly as they normally would. There’s no instrumentation to alter how the athlete moves, so the awkwardness or restriction a marker setup introduces is gone, and the movement being captured is the movement that actually occurs.
While the athlete runs the assessment, multi-camera video records the session, and Theia3D's deep-learning model translates that video into a 3D kinematic dataset of every movement captured.
Each sport-specific movement maps onto kinematic variables the skeletal model can measure directly. For example:
- Cutting and change of direction become measurements of knee valgus angle, trunk lean, and ground contact time, synchronized with force plate loading.
- Deceleration becomes a measurement of knee flexion and joint loading across the braking step.
- Vertical and lateral jumps become measurements of inter-limb takeoff and landing asymmetry and joint power contributions.
- Running and acceleration become measurements of hip and knee kinematics, stride asymmetry, and spatiotemporal gait parameters.
- Single-leg balance becomes a measurement of center-of-mass sway and pelvic drop.
Captured this way, each test yields a consistent set of kinematic measurements that a practitioner can examine alongside their own observation of the movement. The measurement layer is generated by the model from the recorded video, which gives practitioners objective data to compare across staff and across sessions, while the scoring and interpretation of the assessment remain the practitioner's responsibility.
Because Theia3D is a generalized neural network, it doesn’t require additional data for unique movements, environments, or outlier athletes. A practitioner can run a published protocol, such as a 505 change-of-direction test or a standardized single-leg landing task, or design their own battery, and Theia3D captures the same kinematics either way, whether the assessment is off-the-shelf or custom.
As with any biomechanical system, measurements are not free of variation, and results should be interpreted by a qualified professional.
Translating Synchronized Video Into Research-Grade Motion Data for Analysis
The key landmarks Theia3D tracks are fitted onto a 3D skeleton modeled after user-specified joint constraints. The process is highly precise because our motion analysis software models have been trained on more than 100 million images from 1,000 distinct environments.
The end result is a skeleton with 17 body segments that allows the practitioner to then make precise measurements and observations on the subject, including segment positions, joint angles, and spatiotemporal gait parameters.
Theia3D runs on a local server using consumer-grade NVIDIA GPUs and doesn’t require internet connectivity. Practitioners can save their Theia3D motion data in standard file formats including .C3D, .FBX, or .JSON. Theia3D can also save both raw unfiltered poses and smoothed filtered poses.
No video, participant, or analysis data is ever transmitted to Theia or any external provider, making it a good choice for sports organizations and research institutions with strict participant data privacy and data governance requirements.
Practitioners can also export their data directly into downstream analysis environments such as Visual3D, Excel, Vicon Nexus, Qualisys Track Manager, Python, MATLAB, or another internal athlete management program.
Validated by Independent, Peer-Reviewed Studies
No other markerless system has been validated to the extent of Theia3D as evidenced by more than 50 independent, peer-reviewed studies from leading research institutions that have evaluated the software’s performance.
In a 2025 study published in the International Journal of Sports Physical Therapy, researchers used Theia3D to assess 19 recreational athletes performing single-leg squats and single-leg forward and medial landings across two testing sessions one week apart. The system produced low between-day measurement error and reliably captured the single-leg tasks, supporting its use for repeated movement-data collection and athlete monitoring.
In another 2025 study published in the Journal of Sports Sciences, researchers examined the inter-session reliability of lower extremity joint kinematics and kinetics obtained using Theia3D. They observed 18 healthy participants as they performed six return-to-activity movement tasks across two sessions, and found Theia3D exhibited moderate-to-excellent reliability with minimal session-to-session variation for kinematics.
Repeatability has also been evaluated over longer time intervals. A study published in the Journal of Biomechanics used Theia3D to assess knee osteoarthritis patients across three clinical visits averaging eight days apart, and the researchers found highly repeatable gait outcomes between sessions, with joint angle variability lower than what is typically reported for traditional marker-based methods, where inconsistency in manual marker placement is a known source of measurement error.
This directly addresses the issues that arise with recovery research and sport-specific movement assessments at roster scale. Practitioners need to know whether movement measurements are genuinely changing across sessions before they factor that data into return-to-training readiness, load-management, or longitudinal-monitoring decisions, which remain the practitioner's to make.
As with any biomechanical system, Theia3D should be validated for the specific task, joint, and movement plane needed for a given application, rather than assumed to be equally accurate in every use case.
The NBA: Sport-Specific Movement Assessment
In 2025, the NBA launched a league-wide biomechanics program, installing motion capture labs in the training facilities of all 30 teams within a single year. The program is codified in the current collective bargaining agreement and is scheduled to run at least through the end of the agreement in 2030.
The program is a multi-vendor partnership. Qualisys provides the Miqus Video Plus markerless motion capture cameras, Bertec provides the force plates, BreakAway Data provides the dashboards and visualizations, and Theia3D is the analysis software that converts the synchronized multi-camera video into kinematic data. P3, the private biomechanics facility that has independently evaluated roughly 70 percent of current NBA players, consults to the league on protocol design.
In consultation with the National Basketball Players Association (NBPA) and with sports medicine and performance experts, the NBA developed protocols for a screening program that requires athletes to participate in up to four assessments per season. These assessments are expected to take about 15 minutes each and follow a pre-scripted set of motions.
As Theia CEO Marcus Brown put it, “Theia3D is an accessible tool that also enables standardization within a vast data set. As a generalized neural network, Theia3D doesn't require additional data for unique movements, environments or outlier athletes.” This capability allows the NBA to produce population-level reports for the players’ union. The kinematic data coming from the software will be identical and consistent, regardless of which team or staff member captured it.
Because the underlying kinematic data is captured consistently regardless of which team or staff member recorded it, it can support leaguewide benchmarking, and individual teams can factor their own players' data into training-load and strength-programming decisions made by their performance and medical staff.
Evaluate Theia3D for Your Movement Assessment Workflow
See how Theia3D can help your team capture your sport-specific movement assessments with objective 3D kinematic data, without markers, wearables, or special clothing. We’ll walk you through what a markerless FMS workflow could look like in your facility, including camera setup, capture requirements, data outputs, and downstream analysis options.
Contact our team to discuss your screening workflow.
Disclaimer: This article summarizes motion analysis approaches for research and performance applications. Theia3D is a motion analysis software platform and is not intended to diagnose or treat medical conditions. Interpretation and application of results are the responsibility of the user.